
Extensive changes have been made to the CPT codes for reporting hernia repairs effective January 1, 2023. This section needed to be revamped to reflect current clinical practices utilized in these procedures.
Here is a quick peek at the structure of the new codes:
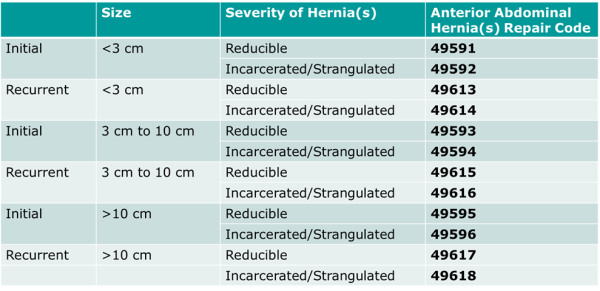
Key points include:
- The new codes identify anterior abdominal hernia repairs by initial vs. recurrent and incarcerated vs. reducible, and by size of defect.
- Procedures that are performed by open, laparoscopic, and robotic approach are all represented in the new codes.
- CPT code 49568 for reporting implantation of mesh has been deleted. The work associated with mesh implantation is now incorporated in the work reported with these new codes.
- All hernias described as epigastric, incisional, ventral, umbilical, and spigelian are now coded with these new codes for anterior abdominal hernia repairs.
- Hernia repair procedures performed on inguinal, femoral, parastomal, and pelvic floor hernias have their own codes and are not reported with these new codes. If inguinal, femoral, lumbar, omphalocele, or parastomal hernias are repaired at the same operative session as an anterior abdominal hernia, they may be coded separately with a modifier -59 (when appropriate).
Documentation Tip! Hernia measurements are performed either in the transverse or craniocaudal dimension. The total length of the defect(s) corresponds to the maximum width or height of an oval drawn to encircle the outer perimeter of all repaired defects. If the defects are not contiguous and are separated by greater than or equal to 10 cm of intact fascia, total defect size is the sum of each defect measured individually.

Jennifer Cayce, RHIT, CCS, CCS-P, CPC, AHIMA Approved ICD-10-CM/PCS Trainer
Director of Coding Quality & Compliance
As a Director of Coding Quality & Compliance, Jennifer brings over 20 years of health information management, auditing, and coding experience to Haugen Consulting Group.
During her career, Jennifer has served as an inpatient and outpatient medical coder, lead coder, coding supervisor, auditor, and has developed training materials for multiple areas of HIM. Jennifer was integral in the development of web-based HIM education for coders, providers, clinical documentation improvement specialists, case managers, and patient access professionals.
During her time as a coding supervisor, Jennifer experienced a high success rate when appealing RAC and other external audit findings.
At the Haugen Consulting Group, Jennifer coordinates and leads the facility audit team and provides coding expertise and support to clients.

If the hernia defect size is not documented in the surgical note, should you not report one of the new codes since they are based on defect size?
AAPC montly magazine, July 2023, states to default to the smallest size but this does not seem appropriate to me.
Hi Karen,
Best practice, if the provider does not include the defect size in the operative note, would be to query the provider so accurate code assignment can be made and so documentation is complete. Provider education on documentation of the defect size may be necessary to ensure this information is included in the future.
The AAPC article is correct in stating that if the defect size is not able to be obtained then the code for the smallest defect would be the default. However, all efforts should be made to have that information included in the documentation.